
Spiny Projection Neurons (SPN)
Spiny Projection Neurons (SPNs), specifically Medium Spiny Neurons (MSNs), are a predominant type of neuron found in the striatum, which is part of the basal ganglia in the brain.
SPNs primarily release the neurotransmitter GABA (gamma-aminobutyric acid), which is inhibitory. This means they decrease the likelihood of the firing of their target neurons.
Basal ganglia (Image taken from: https://selfhacked.com)
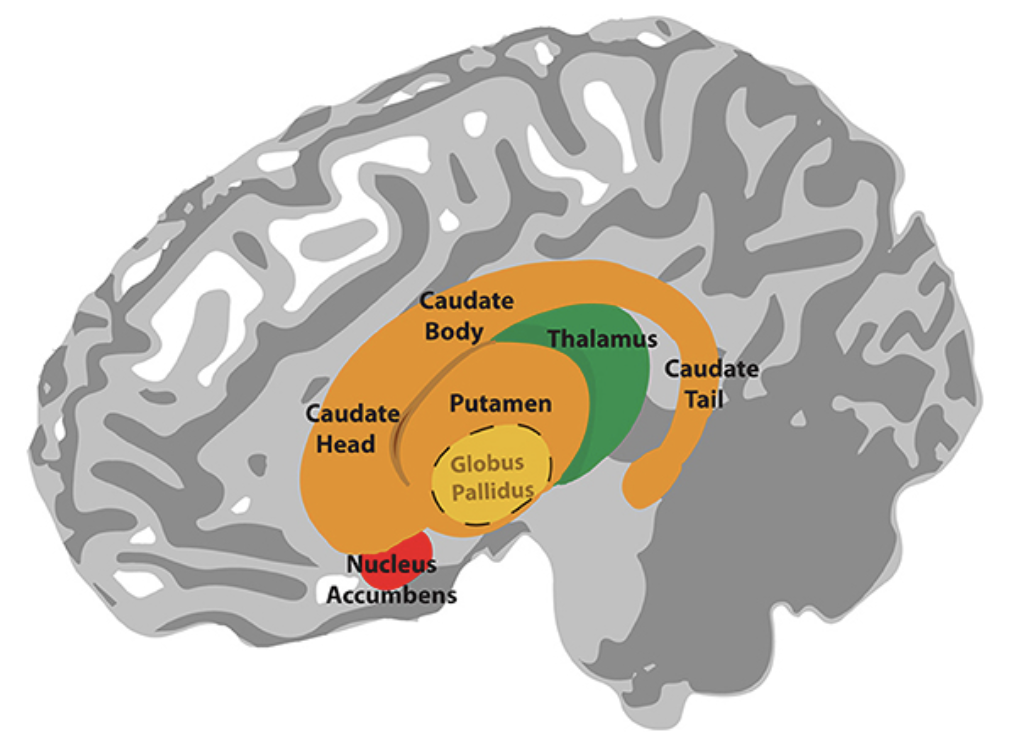 The striatum, the largest structure in the basal ganglia (comprised of the caudate, putamen, and nucleus accumbens as shown above), receives dopaminergic signals from various brain regions and transmits new signals via GABA.
The striatum, the largest structure in the basal ganglia (comprised of the caudate, putamen, and nucleus accumbens as shown above), receives dopaminergic signals from various brain regions and transmits new signals via GABA.
SPNs are classified into two main subtypes based on their projection targets and receptor expression. Direct Pathway SPNs (dSPNs) express D1 dopamine receptors, which respond to dopamine signals from the midbrain, while Indirect Pathway SPNs (iSPNs) express D2 dopamine receptors, which also respond to dopamine but have opposite effects on motor output compared to dSPNs.
Basal ganglia motor circuits (Image taken from: Ferrini A, …, Kurian MA. Mov Disord. 2021).
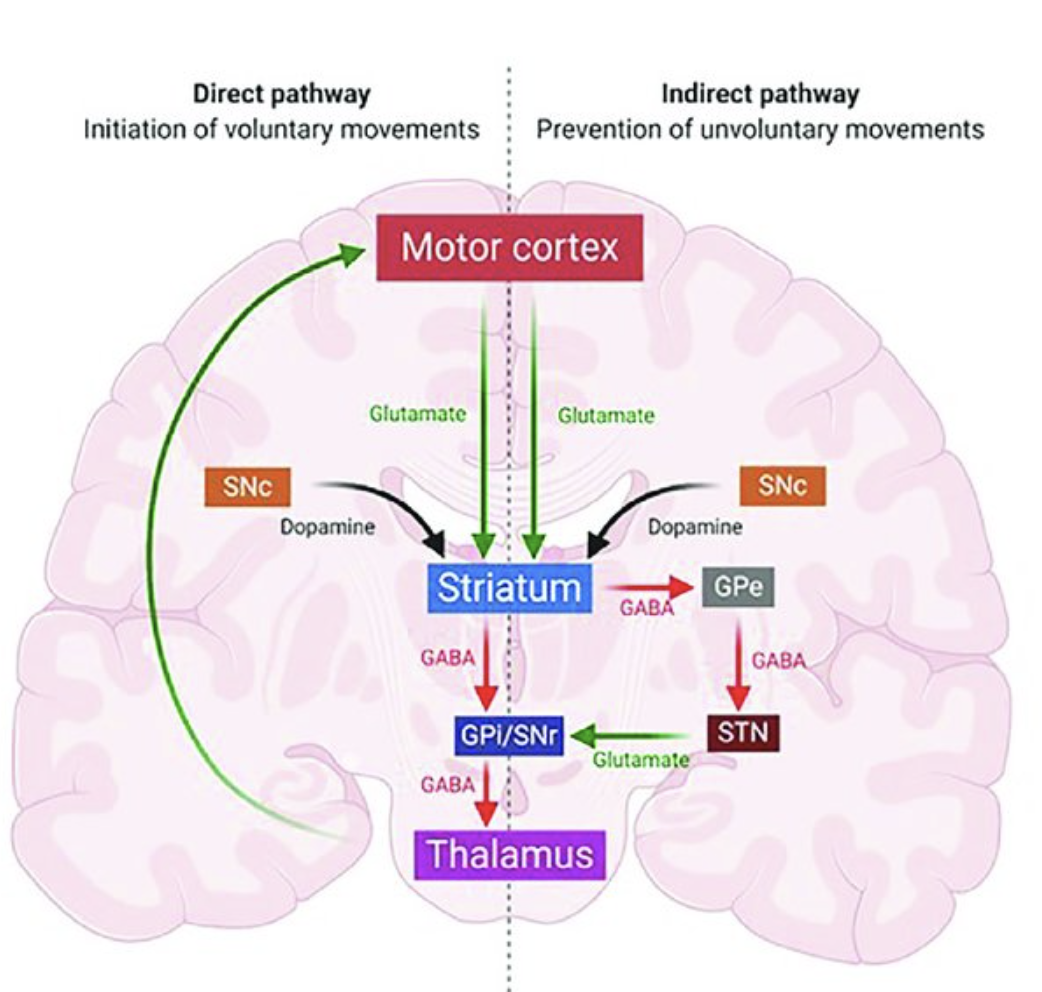
The distinction between dSPNs (direct pathway spiny projection neurons) and iSPNs (indirect pathway spiny projection neurons) is critical to understanding the neural circuits involved in movement disorders like Parkinson’s disease and Dystonia. Here’s a breakdown:
- Direct Pathway (dSPNs):
- Role in Healthy Brain: dSPNs primarily project to the internal segment of the globus pallidus (GPi) and substantia nigra pars reticulata (SNr). Activation of these neurons promotes movement initiation by inhibiting the GPi and SNr, which decreases their inhibitory output to motor areas of the thalamus, thereby facilitating voluntary movement.
- In Parkinson’s Disease: Dopaminergic neuron loss in the substantia nigra pars compacta (SNc) leads to reduced activation of dSPNs. This causes a decrease in movement facilitation, resulting in the characteristic motor symptoms like bradykinesia (slowness of movement).
- In Dystonia: Research suggests that alterations in the direct pathway could contribute to the abnormal involuntary movements seen in dystonia, but the precise mechanisms differ from Parkinson’s disease. Increased dSPN activity has been implicated in some forms of dystonia, leading to hyperkinetic movements.
- Indirect Pathway (iSPNs):
- Role in Healthy Brain: Indirect pathway spiny projection neurons (iSPNs) inhibit movement by activating the external segment of the globus pallidus (GPe), which in turn inhibits the subthalamic nucleus (STN). This results in an increase in GPi and SNr activity, further inhibiting the thalamus and reducing movement.
- In Parkinson’s Disease: The loss of dopamine input also enhances the activity of iSPNs, leading to excessive inhibition of movement. This contributes to the motor deficits observed in Parkinson’s disease, such as rigidity and bradykinesia.
- In Dystonia: While the indirect pathway is also involved in dystonia, the nature of its disruption is different from Parkinson’s disease. Some studies suggest reduced inhibitory control in the indirect pathway could result in excessive movement and the abnormal muscle contractions characteristic of dystonia.
- Dystonia vs. Parkinson’s Disease:
- Dystonia: Primarily a hyperkinetic disorder characterized by sustained or intermittent muscle contractions, resulting in abnormal, often repetitive movements or postures. It’s thought to involve overactivity in the direct pathway and underactivity in the indirect pathway, although this varies depending on the form of dystonia.
- Parkinson’s Disease: A hypokinetic disorder marked by the progressive loss of dopaminergic neurons, leading to decreased movement facilitation via the direct pathway and increased inhibition via the indirect pathway.
The activity of dSPNs must be balanced with that of indirect pathway striatal projection neurons (iSPNs) to maintain proper motor function. This balance ensures that both facilitating and inhibiting signals are appropriately modulated, allowing for refined motor control.
These pathways are essential in motor control, and their dysregulation contributes to the differing motor symptoms in Parkinson’s disease (reduced movement) versus dystonia (excessive, uncontrolled movement).